DrHV FUE
DrHV FUE Protocol
Follicular Unit Excision (FUE) has become the most widely performed technique in hair restoration.
FUE has 4 steps –
- Step 1 – Duration 30 mins – 1 hour ( Doctor step ) Planning and Slit making ( channel making) in bald area – decides direction and density of hair transplant . Duration – 1 hour
- Step 2 – duration 2 – 4 hours – (Doctor step) – Follicular unit excision ( FUE ) from donor area – This step uses punches which cut the skin around the graft. If done incorrectly it can damage the grafts and transect the grafts .
- Step 3 – Duration – 30 mins ( assitant step ) – plucking of grafts from donor area after FUE ( sometimes called Graft extraction to confuse patients ) and counting of grafts
- Step 4 – Duration 2 – 4 hours – (Accepted as assitant step to reduce cost and do more number of grafts in a day ) – Insertion of grafts into holes / channels / slits of bald area which were created by surgeon
According to international defined protocol of hair transplant surgery – slitting ( step 1 ) and graft excision from donor area ( step 2 ) should always be done by doctor himself. These steps cannot be done by nursing staff or assitants or hair technicians.
Indian national board protocol also defines it step 1 and step 2 as surgeon role and high skill job.
While FUE is marketed as a uniform procedure, the reality varies significantly between clinics.
In more than 95 % hair transplant centers in India and Turkey , the most critical part of the surgery—the actual follicular unit excision from donor area ( step 2 as defined above) —is delegated to assistants or nursing staff or unqualified doctors ( trichologist , dentist , ayurveda doctor, homeopathy doctor) or other junior Doctors.
How it impacts your results – Unfortunately hair transplant depends on number of grafts inserted in bald area. It does not depends on additional donor area damage caused by nursing staff . Suppose you require 3000 grafts to cover area. So if a nursing staff attempt on 5000 grafts and damages 2000 grafts and removes 3000 grafts from donor area , then also result will remain good as result is coming due to 3000 grafts implanted. 2000 grafts loss from donor area will not be visible in photos . Total donor area capicity is 6000 – 7000 grafts in your life so now whenever you will need hair transplant – surgeon can remove less grafts from donor area in future. Before and after photos of result in hair transplant surgery are not different. So even if nursing staff removes grafts still you can a good result in before after photos . But It may result in 30 – 80 % additional permanent donar area damage which restrict possibility of future FUE hair transplants. This discrepancy creates a large variation in graft quality, transection rate, donor depletion, and long-term outcomes.
- When patients goes deeper into sugeon role in his hair transplant – More than 50 % hair clinics in India and turkey introduce one of their nursing staff (hair technician / assitant ) as junior doctor or trichologist so that patient thinks that doctor only doing FUE from donor area. But that junior doctor is their actually their staff rather than a doctor.
To address this gap and help patients differentiate high-precision, doctor-performed FUE from mass-produced, technician-driven procedures, we introduce DrHV FUE , a FUE protocol in which all graft harvesting is performed exclusively by the surgeon.
Why a New Term Was Needed
Patients often assume all clinics doing “FUE” are folloing same protocol and technique. However:
The Graft excision from donor area ( FUE ) contributes 70–80% of the surgical impact on the donor area, yet in many clinics it is performed by non-physicians nursing staff , hair technicians , so called trichologists or unqualified doctors.
Marketing practices often highlight only the doctor’s involvement in slits making (a 45–60 minute step) while assistants harvest grafts from donor area for hours.
When patients goes deeper into sugeon role in his hair transplant – More than 50 % hair clinics in India introduce one of their nursing staff or hair technician or assitant as junior doctor or trichologist so that patient thinks that doctor only doing FUE from donor area. They will deny specifically that senior doctor or main doctor will only observe and junior doctor will remove grafts. But that junior doctor is their actually their staff rather than a doctor.
As a result, a clinic may perform 4 -6 surgeries per day on name of a famous doctor , whereas a surgeon-performed FUE practitioner can realistically do 1–2 surgeries in a day.
Patients are unable to understand why graft quality, donor preservation, and long-term safety differ so dramatically.
A distinct, transparent label—DrHV FUE —helps clarify when the harvesting is done by the main surgeon, using controlled parameters and advanced technique to protect the donor.
Why a New Term Was Needed
Patients often assume all clinics doing “FUE” are folloing same protocol and technique. However:
The Graft excision from donor area ( FUE ) contributes 70–80% of the surgical impact on the donor area, yet in many clinics it is performed by non-physicians nursing staff , hair technicians , so called trichologists or unqualified doctors.
Marketing practices often highlight only the doctor’s involvement in slits making (a 45–60 minute step) while assistants harvest grafts from donor area for hours.
As a result, a clinic may perform 4 -6 surgeries per day on name of a famous doctor , whereas a surgeon-performed FUE practitioner can realistically do 1–2 surgeries in a day.
Patients are unable to understand why graft quality, donor preservation, and long-term safety differ so dramatically.
A distinct, transparent label—DrHV FUE —helps clarify when the harvesting is done by the main surgeon, using controlled parameters and advanced technique to protect the donor.
DrHV (FUE) – Why it helps patients :
✓ 100% surgeon-performed graft harvesting
The surgeon performs all extractions, ensuring refined hand control, depth regulation, and real-time decision making.
✓ Micro-regulated punch movements
Sub-millimeter adjustments in:
Angle
Speed
Depth
Torque
Rotation
Minimize follicular trauma, especially in complex donor regions.
✓ Low-voltage, low-RPM, optimal-torque motorized system
Custom settings that reduce frictional heat, torsional stress, and root avulsion.
✓ Maximum donor preservation
Lower transection rates translate into fewer grafts removed to achieve the same cosmetic result.
✓ Tailored extraction pattern
Surgeon-guided scoring maintains uniform density, avoids over-harvesting zones, and protects future transplant options.
Why assitant or nursing staff or hair technician or less qualified surgeon should not extract grafts
Technical reasons
FUE requires continuous tactile feedback, which only an experienced surgeon can interpret.
Assistants / hair technician / nursing staff / less competent doctor may not fully understand variations in:
Graft curl
Splay
Exit angle
Skin thickness
Scar tissue
Lack of judgment leads to:
High transection
Donor overharvesting
“Moth-eaten” appearance
Fewer usable grafts for future procedures
- 30 – 80 % more donor area damage to harvest same number of grafts from donor area
- Donor area damage is permanent
Ethical reasons
Patients believe the doctor is performing the procedure they paid for. DrHV ensures ethical transparency and builds trust. Ideally surgeon should do this step himself in Indian National board or US national medical board protocol but greed and non regulation has lead to this practice of delegating graft excision from donor area to assitant – damaging donor area permanently just to save surgeon time and increase revenue .
Situations Where DrHV Is Especially Superior
Curly or wavy grafts
Thin skin or thick dermis
Previous FUT or FUE scarring
Low donor density
Asian hair with acute exit angles
Afro-textured hair
Repair cases
When these cases are handled by assistants, the donor can be damaged severely. DrHV mitigates these risks.
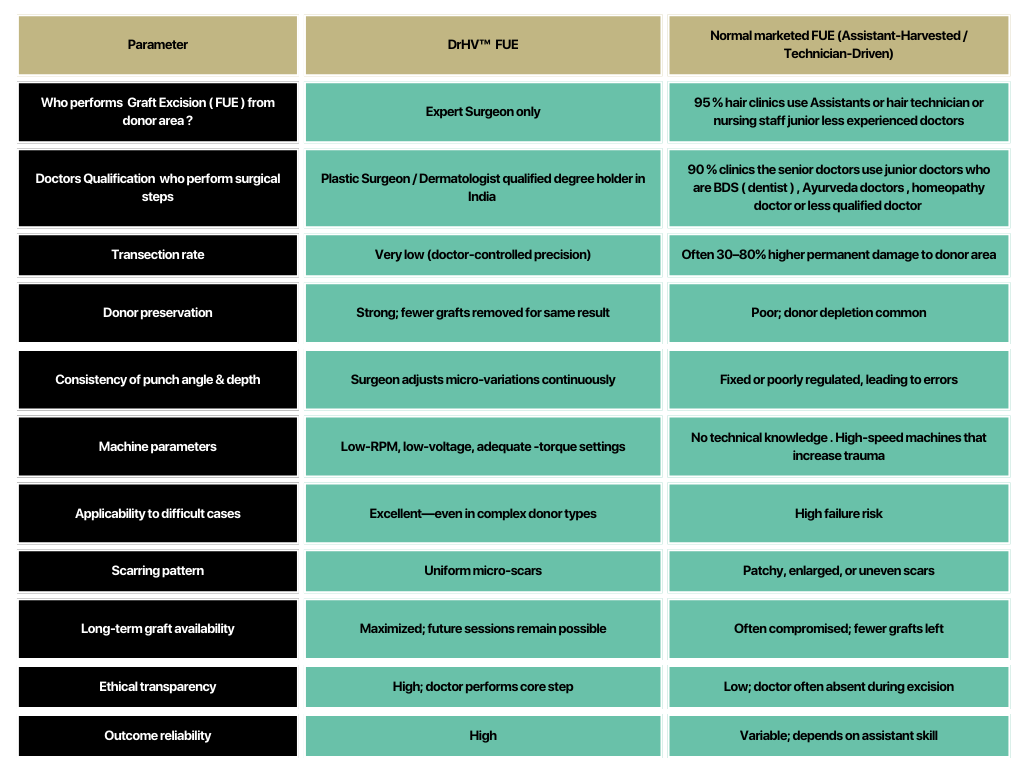
Comparison Table: DrHV FUE vs Standard normal FUE
Key Advantages of DrHV
Better graft survival
Minimal donor trauma
More natural long-term results
Protection of donor for future procedures
Higher overall surgical safety
Ethical surgeon involvement throughout the procedure
Superior results in challenging donor anatomies
DrHV FUE can be combined with better techniques
1. MAGP technique – A Microscope is used during graft extraction so that more thicker and garfts with more number of hairs are extracted from your donor area. This technique provides you with the best quality grafts among all the available methods of Graft Extraction. Read more about MAGP Hair Transplant here
2. DHT Technique – In this technique, we try to place grafts as soon as possible after their extraction from your donor area. Read more about Direct Hair Transplant here.
3. Implanter pen Insertion of grafts – AKESO CHI – In this technique, grafts are inserted with the help of the Choi implanter. AKESO also provides Implanter pen insertion of Grafts We create slits first before placing grafts by CHOI IMPLANTER PEN. It provides more control over the direction and density of hair transplant. Click here to read more about AKESO CHI
Natural looking hair transplant results
Natural looking Results with high density hair transplant






Heartfelt Testimonials from Smiling Faces Everywhere
4.5 Customer Reviews
EXCELLENTTrustindex verifies that the original source of the review is Google. Want to share my own experience regarding Akeso hair transplant is unbelievable.. though I was scared about treatment or result but when I had this in last may 2024 it was wonderful treated by Doctor Akhilesh and their staff.. after two or three months I saw the result as proper new hair what I didn't expect,. Today after seven or eight months there is full growth of hair on all transplanted area. I suggest to all viewers visit 'Akeso Delhi India' once and experience the truth.Posted onTrustindex verifies that the original source of the review is Google. I was searching for the best hair transplant options in India and eventually decided to visit Akeso Hair Transplant Clinic,Delhi , traveling all the way from Kolkata. I received exceptional care from Dr. Akhilesh, who is highly skilled in this field. Three days ago I have finished my hair transplant in Akeso . The main reason I choose Akeso Hair Transplant clinic for my transplant is that the role of doctor in the hair transplant procedure is maximum in Akeso compared to other hair clinic . The staff at the clinic was very professional and attentive, ensuring that I felt comfortable throughout the entire process. I highly recommend Akeso Hair Transplant Clinic to anyone considering a hair transplant; their expertise and commitment to patient satisfaction truly set them apart.Posted onTrustindex verifies that the original source of the review is Google. Authentic place, The doctor was very good and the entire procedure was done by him.Posted onTrustindex verifies that the original source of the review is Google. I had my hair transplant done last year in July for 2500 grafts. After that, I had been on medication. I am completed satisfied with my hair growth result. I recommend everyone to visit Akeso hair transplant centre.Posted onTrustindex verifies that the original source of the review is Google. Thank you so much for the hair Transplant. I have got 3500 grafts transplanted done by Dr.Akhilesh Jangid. I am from Hyderabad and little hesistant to visit Delhi. I tired to look for clincs in my city but doesnt noted any clincs which use new technology like Microscopic and implanters, which improves the result. I noted that Akesko clinic using this technology. The role of doctors in this Hair Transplant is more when compared to other clinic. Initially, I was unsure about the process, whether it's painful or how much is the sucess rate. But, After talking to Akhilesh Jangid (3 times through video consultation) and reading the reviews, I got confidence in the process. The hair transplant went very smooth and before performing, each step is explained. I am very thankful to Doctor and staff, they are very polite and helpful in answering my all questions throughout my hair transplant journey.I personally recommended this clinc.Posted onTrustindex verifies that the original source of the review is Google. Je suis pleinement satisfait de mon intervention chez AKESO. Tout était clair et transparent dès le départ, ce qui m'a amené à effectuer mon intervention chez eux. Le médecin ainsi que ses assistants ont toujours été patients pour expliquer et reexpliquer les choses qui n'était pas clair, dans cette aventure longue et complexe. Un grand merci au Dr Akilesh et à son équipe.Posted onTrustindex verifies that the original source of the review is Google. I have visited Akeso (Dr Akhilesh Jangid) for hair transplant on 10th of June 2024. It's been 6 months now and I have seen significant growth of hair on my scalp. Considering just 3600 implants I am really satisfied with the result. With two free PRPs I am hoping to improve the hair quality even further.Posted onTrustindex verifies that the original source of the review is Google. Akeso is the best option for hair transplant. Dr Akhilesh Jangid is the best hair transplant doctor. I would recommend everyone who wants to or is planning for hair transplant, he or she should undoubtedly go for akeso. Thank you akeso 🙂

